DOES THIS PATIENT HAVE A SEIZURE OR SYNCOPE?
A universally challenging problem facing emergency physicians; this Lancet article sums up the topic very well, in fair detail. (See this reference).
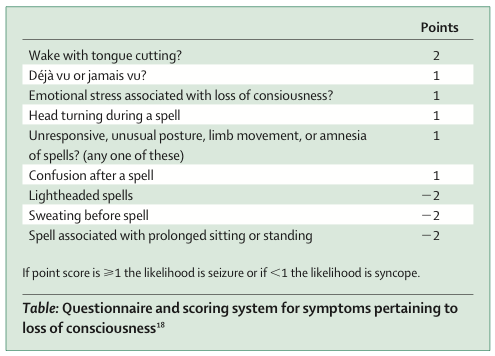
It really boils down to a good history - here is where the eyewitnesses and paramedics are really helpful (sometimes). And no... urinary incontinence doesn't quite help (See this reference). This questionnaire may be useful:
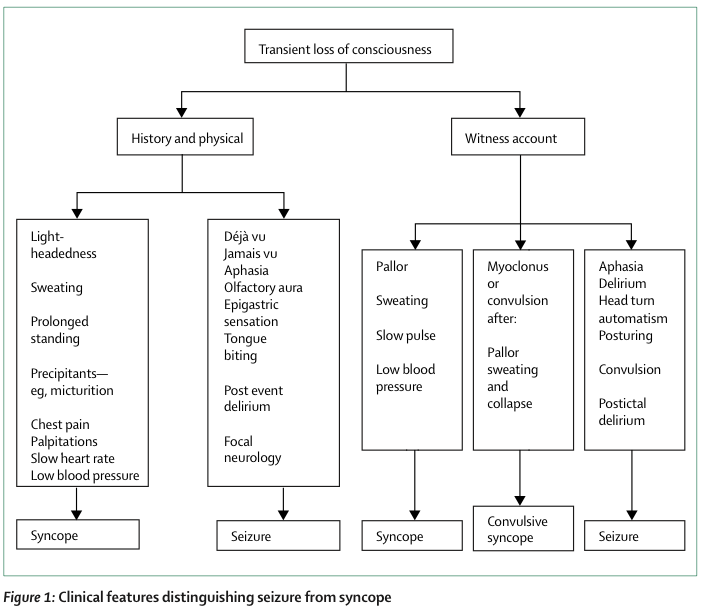
Or this flowchart combining history, physical and eye-witness account:
Convulsions are often seen in syncope as well (convulsive syncope), and are more common than you think (70-90%), but the duration is usually brief.
From LITFL:
Seizure is more likely if:
- Tonic-clonic movements are usually prolonged and their onset coincides with loss of consciousness
- Hemilateral clonic movement
- Clear automatisms such as chewing or lip smacking or frothing at the mouth (partial seizure)
- Tongue biting (especially laterally)
- Blue face
- Prior to the event: aura (such as unusual smell)
- Post-ictal confusion
- Tonic-clonic movements are always of short duration (<15 sec) and they start after the loss of consciousness
- Prior to the event: Nausea, vomiting, feeling of cold, sweating (neurally-mediated)
- short duration
WHAT ABOUT THE USE OF SERUM PROLACTIN IN DIFFERENTIATING SEIZURES FROM SYNCOPE?
Nope, serum prolactin is almost completely hopeless. (See this reference - report form the American Academy of Neurology)
What the article recommends:
- Serum prolactin assay does NOT distinguish epileptic seizures from syncope (in both conditions, serum prolactin are elevated). Level of Evidence B
- Elevated serum prolactin assay, when measured in the appropriate clinical setting at 10 to 20 minutes after a suspected event, is a useful adjunct for the differentiation of generalized tonic-clonic or complex partial seizure from psychogenic nonepileptic seizure among adults and older children. Level of Evidence B
WHAT ABOUT TIA IN PATIENTS WITH SYNCOPE?
A misconception is that transient LOC are commonly due to a TIA. The fact is, to have LOC in TIA/stroke, there must be either bilateral carotid artery disease or posterior circulation disease, in which there must be other accompanying neurological signs and symptoms! (e.g. cerebellar signs)
(See this reference - TIA definition) - What it says:
Syncope: A transient self-limited loss of consciousness, usually leading to falling. The onset is relatively rapid, and the subsequent recovery is spontaneous, complete and relatively prompt. The underlying mechanism is a transient global cerebral hypoperfusion.
Transient ischemic attacks are different in that they represent focal cerebral or retinal hypoperfusion. In general, syncope is brief loss of consciousness without focal neurologic signs or symptoms, whereas transient ischemic attacks are brief focal neurologic signs and symptoms without loss of consciousness.
TIA related to a carotid artery does not cause T-LOC. When almost all cerebral arteries are occluded, transient obstruction of the remaining vessel subtending a large portion of the brain may extremely rarely affect consciousness only in the standing position. Moreover, focal neurological signs are much more prevalent.
TIA of the vertebrobasilar system can cause LOC, but there are always focal signs, usually limb weakness, gait and limb ataxia, ocu-lomotor palsies, and oropharyngeal dysfunction. For all practical purposes a TIA concerns a focal deficit without LOC, and syncope the opposite.
WHAT ABOUT NEURO-IMAGING IN PATIENTS WITH SYNCOPE?
This is a common mis-understanding. Somehow, many doctors think that patients with syncope mandates a CT brain. In fact, European Society for Cardiology guidelines and ACEP guidelines DO NOT recommend routine CT / MRI for syncope. Image only if a seizure is suspected to be the more likely cause.
ALIEM goes on to advise when a CT brain is advised:
Clinicians might consider obtaining a Head CT as part of the syncope evaluation for the following findings:
- Trauma above the clavicle
- Persistent neurologic deficit or complaint
- Age >65
- Sudden onset headache
- Patients on warfarin (coumadin)
WHAT ABOUT THE USE OF SYNCOPE RISK STRATIFICATION TOOLS?
The most well known tools are the San Francisco Syncope Rule and the Boston Syncope Rule.
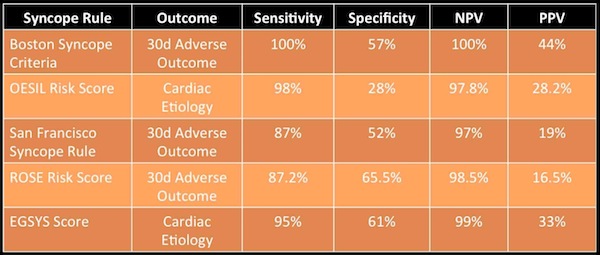
This is from ALIEM post on Management of Syncope, it is a good read. What do they say?
Bottomline: "Educated clinician judgment based on EBM guidelines (European Society for Cardiology and ACEP) seems to be the best strategy for management. Syncope prediction rules can certainly aid this process, but they do not yet fit for use alone for risk stratification in any population."
I generally agree with that, and don't use any form of risk stratification tool for syncope. If you do use the SFSR for example, use it as an adjunct to clinical judgement. So what then? See below...
SO WHAT DO I DO WITH THAT PATIENT WITH SYNCOPE?
In my opinion, I like what Dr Smith's ECG blog has laid out, and more recently on emDocs as well. What they say also follow fairly closely what ACEP guidelines recommend. In fact, all you really need is HISTORY, PHYSICAL and a good read of the ECG! (Dr Smith's post is longer than mine, and contain very valuable info, references to this topic). After that, it is about a GOOD CLINICAL ASSESSMENT and investigating for what you think the likely causes are.
Only last month in Aug 2015, ESC published a consensus syncope risk stratification in the emergency department. (See this reference). A very simple conceptual flow chart:

A short 6 page article well worth your time and to think about.
Web References
No comments:
Post a Comment